Rewriting Life
Cell Type Counts in Spinal Therapy
Rats regain motor skills with one kind of cell transplant, get nerve pain with another.
Small differences in the type of cells used for transplantation therapies can have a big impact on outcome. In experiments published in the current edition of the Journal of Biology, scientists from the University of Rochester and the University of Colorado found that transplanting a certain type of cell improved motor function in rats whose spinal cords had been severed. However, transplantation of a closely related cell type had little benefit and actually made the animals more sensitive to pain.
The findings illustrate the importance of differentiating stem cells before transplanting them into injured tissue, an issue that has been under great debate as stem cell-based therapies approach human testing. “This study demonstrates for the first time the dynamics of developmentally different populations of [cells], which we need to take into account,” says Martin Marsala, a professor of anesthesiology who teaches at the University of San Diego and was not involved in the study.
Stem cells have the potential to grow into new neurons and other cell types, a property scientists aim to exploit to treat spinal cord injury. Transplanted cells might bridge severed nerves in the spinal cord or encourage recovery of existing cells. However, scientists working toward this goal have run into two main problems: stem cells transplanted into the spinal cord have a hard time forming lasting neurons, and these same cells tend to induce nerve-related pain.
One problem is that transplanting undifferentiated, or “naïve,” stem cells into injured tissue cells tends to cause the formation of scar tissue, instead of regenerating healthy neurons, says Stephen Davies, associate professor of neurosurgery at the University of Colorado. “It might be that scars form to protect an injury site from infection, so the injured tissue goes into lockdown mode and will recruit whatever precursor cells are present to form scars,” he says. The alternative is to differentiate cells into specific cell types before transplanting them.
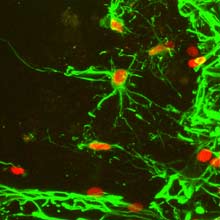
Davies and his associates at the University of Rochester found that the right kind of cells for repairing spinal cord injuries may be a subtype of support cells found throughout the central nervous system, called astrocytes. These star-shaped cells have various forms and functions, but are largely involved in providing nutrients to the brain and repairing injury.
To test their healing potential, Davies’ team grew two different kinds of astrocytes from the same line of embryonic stem cells by exposing them to different cocktails of signaling molecules–molecules that stimulate stem cells to grow into specific cells. One sample yielded astrocytes that were flat and broad, called GDAbmp. The other produced more elongated astrocytes, called GDAcntf.
The researchers then surgically severed rats’ spinal cords at the base of the neck–a common location of spinal injury in humans–and injected the animals with naïve stem cells, stem cell-derived GDAbmp, and stem cell-derived GDAcntf.
Every three days after surgery, the researchers tested the rats’ ability to walk across a horizontal ladder. They found that the rats that received GDAbmp injections quickly recovered motor skills and were able to walk across the ladder as well as they could before the surgery. By contrast, the rats injected with GDAcntf or with naïve stem cells showed no statistically significant recovery, similar to rats that received no injection at all.
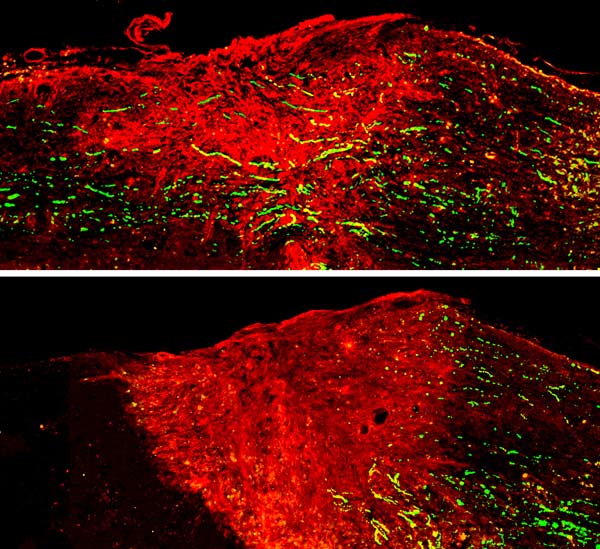
Images of each injury site after cell injections showed that GDAbmp astrocytes promoted the regeneration of severed nerve fibers across spinal cord injuries while the GDAcntf and naïve stem cells did not.
In addition, Davies’ colleague and wife Jeannette Davies discovered that rats with injected GDAcntf astrocytes were much more sensitive to pain than rats with GDAbmp astrocytes. Furthermore, in histological samples, the team found that rats with GDAcntf exhibited sprouting of nerve fibers associated with neuropathic pain, whereas rats with GDAbmp did not show such sprouting.
“So far, these [GDAbmp astrocytes] are the gold standard astrocytes that have been discovered,” says Davies. “Not only do they not promote neuropathic pain, but they have robust regeneration of neurons, and [they lead to] locomotor recovery in two to three weeks.”
Davies says manipulating stem cells before transplanting them into injured sites may have beneficial effects not just for repairing spinal cords, but also for treating injuries in other parts of the body. For now, he and his team are exploring methods to make GDAbmp for humans, either from embryonic stem cells or from adult stem cells, with a view toward transplanting these cells into humans in clinical trials in the next two or three years.