Rewriting Life
Pig-to-Monkey Transplant Treats Diabetes
Embryonic tissue could let xenotransplants evade the host’s immune system.
Using embryonic tissue for interspecies organ transplants offers a way to evade the host’s immune system, say scientists who used the method to treat type 1 diabetes in primates. By transplanting embryonic pancreatic tissue from pigs to monkeys, Israeli researchers report that they were able to reverse the primates’ insulin deficiency.
The key, the researchers say, is the embryonic tissue’s ability to grow into a new pancreas that uses blood vessels from the host animal. The host blood vessels are not subject to the dangerous immune reaction that has always dogged xenotransplants of mature pancreatic material.
The research team, led by Yair Reisner of the Weizmann Institute, claims that the results, published in the latest issue of the journal PNAS, could offer an attractive replacement therapy for type 1 diabetes, an autoimmune disease in which the destruction of the pancreas means that sufferers rely on injections of the hormone insulin to control their blood-sugar levels.
In an earlier study, the researchers found evidence that semiformed pancreatic tissue taken from pig embryos at 42 days of gestation appeared to offer the best combination of characteristics for xenotransplantation. According to Reisner, if they’re harvested too early, there may not be enough partially differentiated pancreatic cells. But if taken too late, the tissues’ ability to grow into a new organ is diminished, perhaps because they contain too few stem cells, while their ability to cause immune rejection increases.
In the latest study, the researchers transplanted 42-day-old pig pancreatic tissue into monkeys with induced type 1 diabetes. The first pair of animals involved in the study died soon after transplantation from an infection caused by too much immunosuppressive therapy.
The second pair of animals received milder immunotherapy and survived for a year. Furthermore, within five months of treatment, the animals had grown new pancreases and were no longer reliant on insulin injections. This indicates that the replacement organs had sufficient islets–tiny, insulin-producing structures consisting of around 1,500 beta cells, which have their own intricate vascular systems.
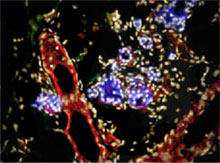
Radioimmunoassay tests confirmed that the insulin produced by the monkey was porcine, while the network of vessels running through the new organ was made of host cells. “This is important because it meant the monkey’s immune system did not attack the vessels,” says Reisner.
This type of immune reaction has been a bugbear for researchers, he says, because primates, including humans, produce a class of antibodies that attack the sugar molecules that coat pig blood-vessel tissue.
Significant immunosuppressive therapy is still needed to reduce other types of host immune reaction against the pig pancreatic cells. But Reisner claims that this is at the level typically seen in transplant medicine–even though the researchers report that both animals died from infections and drug toxicity a year after their transplants. He adds that there is scope for further reducing the amount of therapy required. “We’re fine-tuning things to reduce the levels of toxicity,” he says. “The important thing is that we set out to show that a pancreas could be grown this way, and that it could correct the uncontrolled glucose levels caused by diabetes, which is what we’ve done.”
Reisner believes that the technique could eventually help humans with the same condition. Human-to-human pancreatic transplants have been shown to be effective, but a lack of donors severely limits the number of such treatments available. “The purpose of this study was to show that we could potentially have a method of providing an unlimited source of transplantation for treating diabetes.”
However, Reisner, who is a scientific consultant and holds equity with Tissera, which supported the research, says that much work needs to be done before the xenotransplantation method can be used clinically.
Gordon Weir, head of the Islet Transplantation and Cell Biology Center, at Harvard Medical School’s Joslin Diabetes Center, says that it is too soon to write off sources other than 42-day-old embryonic tissue for growing new islets. “I’m not necessarily convinced by the 42-day number,” he says. “Some people have had good results with neonatal tissue.” He adds that even mature pancreatic transplant tissue can become infiltrated to some extent by host blood vessels.
Other approaches to reversing type 1 diabetes are also emerging. Of particular interest are methods that seek to reprogram a patient’s immune system to stop it from attacking the pancreas. Recently, it was reported that destroying pancreas-killing immune cells and replacing them with a patient’s own stem cells can help her gain control over blood-sugar levels.
A more extreme approach is to completely wipe out a diabetic’s immune system and rebuild it using his bone-marrow stem cells–a strategy that has raised some safety concerns.
“This is an interesting approach that seeks to avoid transplants,” says Reisner. “It could work if used early on in the disease, while the patient still has some pancreatic tissue. But later on, when all the beta cells are destroyed, an alternative approach like ours might have to be used.”
Weir adds that “terrific progress” has been made in harvesting stem cells to make new pancreatic tissue and that he is hopeful that before long this will translate into major clinical breakthroughs.